Dr. Alex Ong
Optometrist and Certified Personalised Nutritional Practitioner (CPNP), Singapore
Abstract
If we look back just over a decade, the landscape of eye care looked drastically different. Myopia Management was a niche interest, often relegated to the sidelines of standard practice. Today, it is a global imperative. The fact that Myopia in children has gained such massive attention is an undeniable success story for our profession; we have successfully alerted the world to the problem. (1)
But as we celebrate this awareness, we must ask a harder question: “Are we doing the right thing in how we educate parents and manage these children?”
For years, we have relied on the phoropter as our primary tool. We chase the number on the prescription, trying to “hold back the dioptres.” But as we shift from simple vision correction to pathology prevention, we must confront a fundamental clinical reality: refraction is often a poor proxy for the true anatomical state of the eye. (2)
The Clinical Dilemma: Three Children, Similar Prescriptions
To illustrate this, let us consider a scenario involving three real-world cases: KF, SQ, and SO.
Imagine these three children sit in your chair with moderate Myopia ranging from -3.00 D to -3.75 D. Based on refraction alone, they appear clinically similar. They would likely receive the same explanation and perhaps the same treatment urgency. However, when we look “under the hood” with ocular biometry, the risk profiles diverge dramatically.
1. KF: The “Refractive” Myope
- Refraction: ~ -3.00 D
- Axial Length (AXL): 23.03 mm
- Corneal Curvature (K): Steep (~47.00 D)
- Analysis: KF’s eye is not abnormally long. His Myopia is driven almost entirely by his very steep corneas (>47 D). His risk of retinal pathology associated with elongation is relatively low.
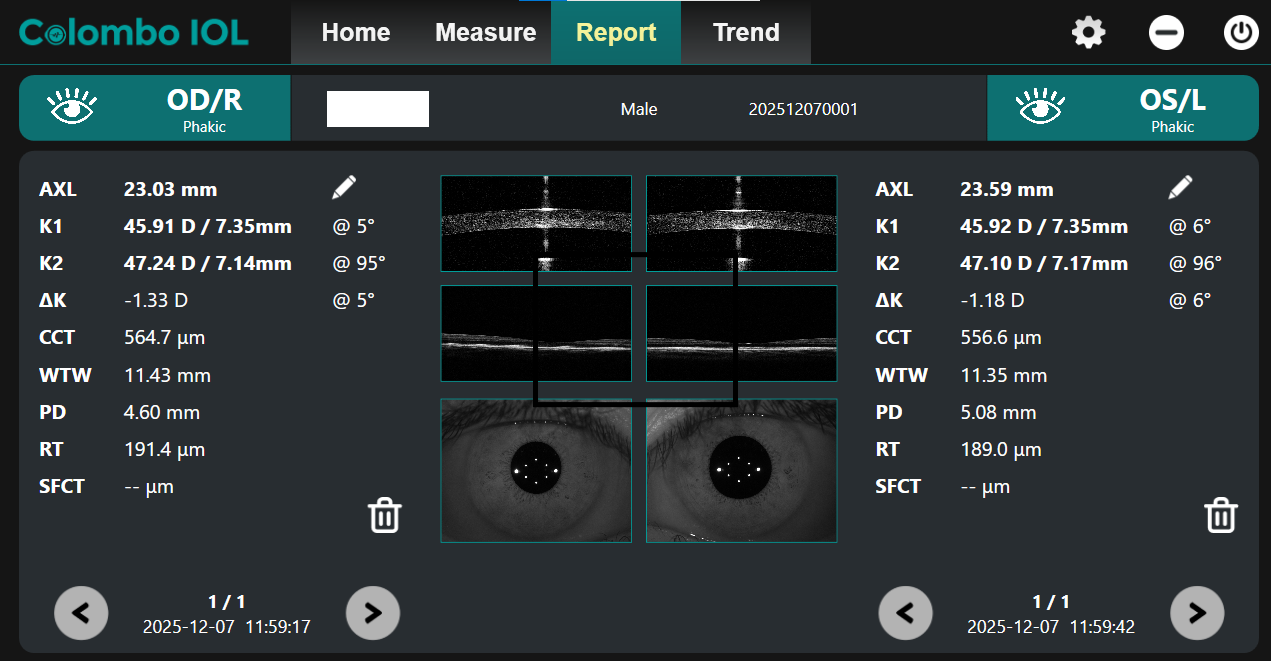
Figure 1: Image showing axial length measurement of KF
Image Courtesy: Created by Author
2. SQ: The “Standard” Myope
- Refraction: -3.75 D
- Axial Length (AXL): 24.48 mm (OD) / 24.72 mm (OS)
- Corneal Curvature (K): Average (~45.00 D)
- Analysis: SQ represents the “textbook” myope. Her corneal power is standard, and her axial length (~24.5 mm to 24.7 mm) correlates well with her -3.75 D prescription. She requires management, but her anatomy is consistent with her refractive error.
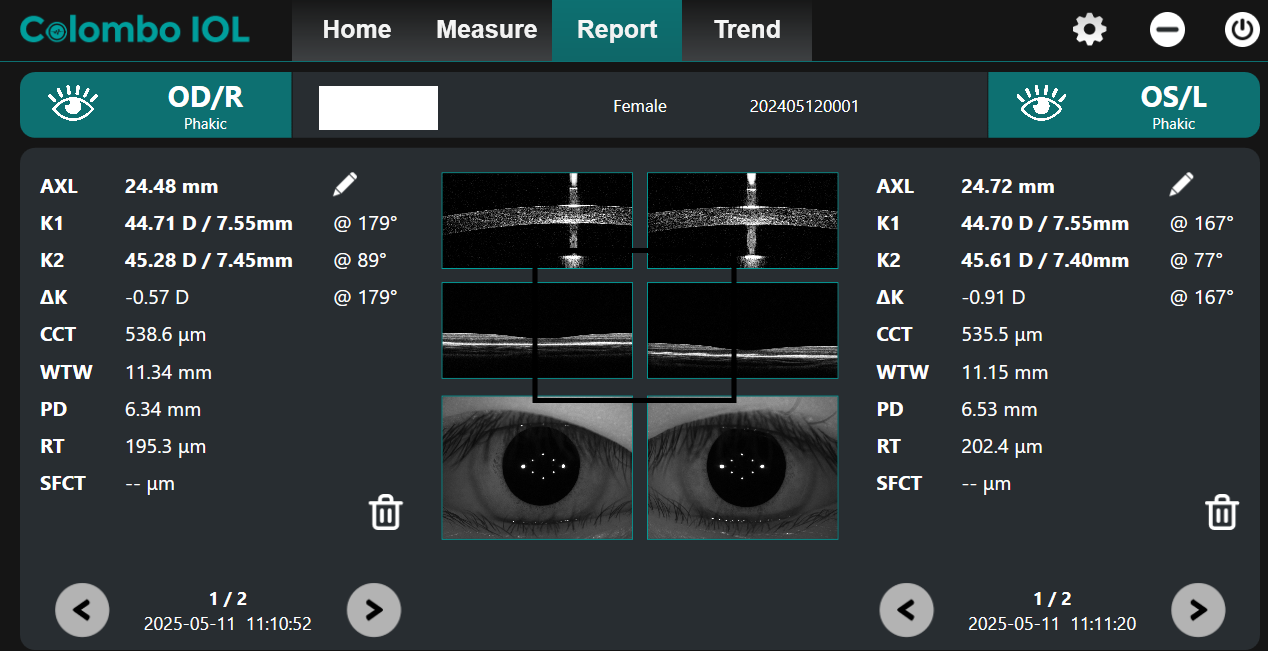
Figure 2: Image showing axial length measurement of SQ
Image Courtesy: Created by Author
3. SO: The “Silent Risk” (The Flat Cornea Phenotype)
- Refraction: ~ -3.50 D
- Axial Length (AXL): 26.37 mm (OD) / 26.06 mm (OS)
- Corneal Curvature (K): Flat (~39.78 D)
- Analysis: SO represents the most dangerous clinical profile. Her corneas are incredibly flat (under 40 D). To result in a moderate prescription with such weak corneal power, her eye must be exceptionally long to compensate.
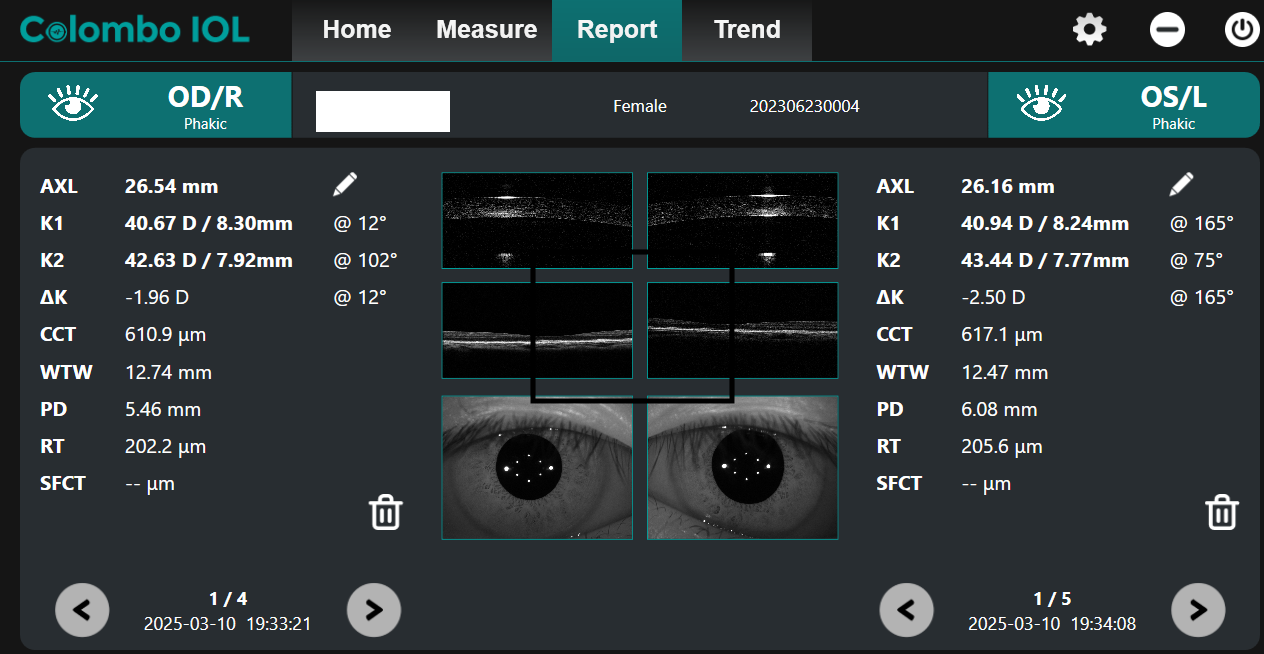
Figure 3: Image showing axial length measurement of SO
Image Courtesy: Created by Author
The “Guessing Game” of K-Readings: Can We Calculate Axial Length?
This brings us to a critical gap in standard care. Many practitioners ask: “If I have the refraction and the K-readings from my standard autorefractor/keratometer, can I not just calculate the axial length?” The answer is yes, but with a major warning label.
Research by Morgan et al. has shown that it is possible to estimate axial length using corneal curvature and refractive error with reasonable accuracy for risk stratification. The derived formula allows practitioners without a biometer to estimate if a child is in the “danger zone” (e.g., >26 mm). (8)
However, for Myopia Management, this calculation has a fatal flaw: Precision. Morgan et al. found that the 95% confidence limits for this calculation are approximately ±0.73 mm. In the context of Myopia Control, where we are fighting to stop 0.1 mm or 0.2 mm of annual growth, an error margin of nearly 0.75 mm is unacceptable. As the authors conclude, while the formula is useful for an initial “snapshot,” it is “too noisy to be employed for precise tracking of Myopic changes over time”.
The Clinical Takeaway:
- If you do not have a biometer: Use the Morgan et al. formula to estimate risk at the first visit. If the calculated length is high, refer or treat aggressively.
- If you are managing Myopia: You cannot rely on calculation to see if your treatment is working. You need physical measurement.
Redefining the Standard of Care
We must stop treating numbers and start treating anatomy. The “success” of Myopia Management’s popularity is only the first step; the next step is precision.
- Biometry should be the New Gold Standard: We cannot assess true risk without knowing the AXL/K relationship. As highlighted in recent literature, axial length is a far better predictor of future disease risk than refraction. (4)
- Watch the Ks: If you do not have a biometer yet, you must at least monitor the K-readings. If you see a Myopic child with flat Ks (<42 D), red flags should wave. This is likely a long eye in disguise.
- Educate on “Size” not “Power”: We need to teach parents that we are treating the size of the eye, not just the thickness of the glasses.
The Flat Cornea Dilemma: Why Standard Options Fail
For a patient like SO, urgency is paramount. The higher the axial length, the fewer “safe” years we have left to intervene. Furthermore, her specific anatomy, extremely flat corneas, complicates standard treatments:
- Orthokeratology Limitations: Ortho-K relies on compression factor. With a cornea as flat as 39D, there is a physiological limit to how much flatter we can make it. We may not be able to fully correct her prescription or generate the necessary peripheral defocus to halt elongation.
- Soft Contact Lens Instability: Most commercial soft lenses for Myopia control are designed with base curves (e.g., 8.3–8.7 mm) suited for average corneas. On a flat cornea like SO’s, these lenses may be too steep, leading to excessive tightness, discomfort, making them unsustainable for long-term wear.
A Clinical Action Plan for the High-Risk Myope
- Deploy the Highest Tier of Treatment Immediately: Do not start with “entry-level” options. We must choose the method with the highest statistical success rate available in the clinic. If optical options are limited by corneal shape, pharmacological intervention (Atropine) or specialized custom lens designs must be prioritized. (4)
- Implement a 3-Monthly Review Cycle: Standard 6-month recalls are insufficient. It should be recommended to shorten the follow-up loop to catch progression early. If the axial length continues to sprint, it should be picked up within 12 weeks, not 24.
- Set a Progression Target: According to international guidelines, success in the management should aim to mimic physiological emmetropic growth. A realistic target is to keep axial elongation below 0.2 mm per year. (5)
- Combination Therapy is Key: If the primary method shows only partial success and the target is not met, do not hesitate to add a second modality. Combination therapy (e.g., Atropine + Defocus Spectacles) is often necessary for rapid progressors.
Beyond the Phoropter: A Holistic Approach
While lenses and drops are powerful, they are not the only tools in our arsenal. We must treat the child holistically, considering all modifiable risk factors.
- Light and Dopamine: “Light” must be prescribed just as we prescribe lenses. The mechanism is now well-understood: bright outdoor light stimulates the release of retinal dopamine. Dopamine acts as a critical “stop signal” or brake for axial elongation. Without sufficient outdoor light intensity (aiming for 2 hours daily), dopamine levels drop, removing the natural inhibition on eye growth. (7)
- Visual Diet (Near Work): It is not just about reducing screen time, but managing the working distance (>30cm) and taking breaks. The intensity of near work is a major driver of elongation. (5,6)
- Nutrition: Emerging evidence suggests a link between diet and ocular health. Ensuring a diet low in processed sugars and high in whole foods may support the scleral structure and overall circadian rhythm, which in turn influences eye growth. (6)
Conclusion: The New Standard of Care
As we look toward the future of Myopia Management, it is clear that our definition of “success” must evolve. Eyecare practitioners must shift our focus to anatomy. Children with axial lengths trending toward the pathological danger zone, especially those masking their risk with flat corneas, require our most decisive and aggressive interventions. Whether through orthokeratology, atropine, or combination therapies, our management must always be rooted in evidence-based solutions.
The era of “chasing dioptres” must end; the era of measuring millimetres, ocular biometry should be the new standard of care. Finally, we must remember that we are treating a child, not just an eye. Beyond lenses and pharmacological drops, we must address the modifiable lifestyle factors, from outdoor light exposure and sleep hygiene to nutritional support. These are often the missing pieces of the puzzle.
References
- World Health Organization (WHO) & Brien Holden Vision Institute. The Impact of Myopia and High Myopia: Report of the Joint World Health Organization–Brien Holden Vision Institute Global Scientific Meeting on Myopia. Sydney, Australia: University of New South Wales; 2015.
- Review of Myopia Management. Why Axial Length Matters: The Long and Short of It. Review of Myopia Management. Available online. Accessed 2024.
- Ong ACH. Case Study: Are Axial Length and Refractive Error Always Correlated? Review of Myopia Management. Published October 16, 2023.
- World Society of Paediatric Ophthalmology and Strabismus (WSPOS). Myopia Consensus Statement 2023. WSPOS; 2023. Available at: wspos.org.
- Gifford KL, Richdale K, Faulkner T, et al. International Myopia Institute Clinical Management Guidelines Report. Investigative Ophthalmology & Visual Science. 2019;60(3):M184-M203.
- Ong ACH, Huang R. The Sleep-Vision-Nutrition Triad: A Holistic Approach to Myopia. Review of Myopia Management. Published December 2, 2025.
- Landis EG, Park HN, Chrenek M, et al. Light Signaling and Myopia Development: A Review. International Journal of Molecular Sciences. 2021;22(9):4460.
About the Author

Dr. Alex Ong
Dr. Alex Ong, DOptom, FAAO, CPNP (US) Optometrist, Singapore
PGCert (Anterior Eye Diseases, Cataract and Glaucoma)
PGCert (Retinal Disease Recognition and Co-Management)
MSCO, B.Sc Optom, Dip. Optom
Dr. Ong is the Founder and Managing Director/Optometrist at Ong’s Optics Myopia Management Centre, established in 2005 and 2nd generation owner of Ong’s Optics and Contact Lens Centre, established in 1985. With over two decades of clinical experience, his expertise spans evidence-based Myopia Management, Ocular Nutrition, Binocular Vision, Orthokeratology, and Geriatric Vision Care. He serves as a Key Opinion Leader for Menicon Japan and has taught as an adjunct lecturer at both optometry schools in Singapore. Dr. Ong is actively involved in Optometric education and professional training across Asia. As a Certified Personalised Nutrition Practitioner (CPNP) with the American Nutrition Association, he integrates nutritional science with vision care to promote a proactive and preventive model of lifelong eye health. He is also a member of Ocular Wellness and Nutrition Society.
Recent Comments