



Abhirami E, M. Optom
PhD Scholar, SRM Medical College Hospital and Research Centre, Kattankulathur, India
Dry Eye Disease (DED) is a multifactorial ocular surface disorder that has become a major public health concern, affecting individuals across all age groups. (1,2) The rising prevalence is linked to certain modifiable risk factors like excessive screen time, contact lens usage, poor diet, and environmental exposures (low humidity, pollution, and sun exposure, air conditioning) and non-modifiable risk factors such as age, female gender, genetic predisposition, and autoimmune disorders. (2) Additionally, one of the key factors contributing to DED in recent years is the extensive use of digital devices in academic, professional, and leisure activities. This can lead to reduced blinking rate, incomplete blinks, more exposure to air, and sustained evaporative stress. (3) Over time, these changes can disrupt the tear film homeostasis, ocular surface integrity and accelerate evaporative stress, creating an imbalance that can initiate inflammatory responses and worsen symptoms of ocular dryness. (4.5)
Challenges with Traditional Diagnostic Tests
The tear film is an extremely delicate and unstable structure. The stability can be easily affected by external factors. Even small changes to the ocular surface, such as contact with diagnostic instruments, the application of dyes, and alterations in eyelid position, can alter the tear distribution and composition.
Conventional DED diagnostic methods, such as the Tear Film Breakup Time (TBUT), Ocular surface staining, and Schirmer’s test, have been primarily used in clinical practice for a long time to assess tear film stability, ocular surface integrity, and tear production. However, their invasive approach can induce reflex tearing, destabilise the tear film, and lead to inconsistent test results, thereby reducing diagnostic precision. (6) In the early stages of DED, these invasive tests can disrupt the natural state of the eyes and may miss early signs of DED, making diagnosis more difficult.
Shift Toward Non-Disruptive Assessment
As understanding of ocular surface physiology has advanced, the Tear Film and Ocular Surface Society (TFOS) DEWS III has emphasised the idea of ‘non-disruptive assessment’ where diagnostic tests are designed to maintain the natural tear environment and provide accurate physiological measurements. (7,8) This change is based on the evidence that metrics like tear film breakup time, lipid layer behaviour, tear osmolarity, and blink dynamics are more dependable when measured without mechanical interference. As a result, non-invasive methods such as Non-Invasive Tear Breakup Time (NITBUT), interferometry, meibography, tear meniscus height, and blink pattern analysis have become more effective tools for the objective and consistent evaluation of DED. (9,10) These technologies help clinicians with early diagnosis of DED and differentiate the subtypes of DED with good accuracy, also improving patient comfort and clinical efficiency.
| Technique | Description | Use |
|---|---|---|
| Symptom Questionnaires | -Ocular Surface Disease Index- 6 & (OSDI-6) OR -Dry Eye Questionnaire -5 (DEQ 5) |
DED symptoms and severity screening tool. OSDI-6 cutoff ≥ 4 suggests positive symptoms DEQ 5 cutoff ≥ 6 suggests positive symptoms |
| Non-Invasive Tear Film Breakup Time (NIBUT) | Measures the time taken for the tear film to break down after a complete blink, using reflected Placido mires or keratometry | Assess tear film stability Cutoff ≤ 10 seconds indicates DED. |
| Tear Film Osmolarity Testing | Uses a small tear sample (nanolitre volume) placed on a test card to measure tear salt concentration. | Assess imbalance in the tear film. (homeostasis disruption) Cutoff ≥ 308 mOsm/L |
| Tear Meniscus Height (TMH) Measurement | Assesses the tear volume gathered on the lower eyelid margin, using slit lamp, infrared imaging or Anterior Segment Optical Coherence Tomography (AS-OCT). | Indicates aqueous tear volume (TMH ≤ 0.20 mm suggests aqueous-deficient DED). |
| Tear Lipid Layer Interferometry | Assesses the tear volume gathered on the lower eyelid margin, using slit lamp, infrared imaging or Anterior Segment Optical Coherence Tomography (AS-OCT). | Indicates aqueous tear volume (TMH ≤ 0.20 mm suggests aqueous-deficient DED). |
| Infrared Meibography | Uses infrared light to image the meibomian glands within the upper and lower eyelid. | Assesses the meibomian gland morphology and structural integrity to identify the gland dropout. |
| Blinking Assessmentt | Automated systems can measure blink rate and the proportion of incomplete blinks. | Identifies blinking disorders as a marker of DED and MGD. |
| Ocular Surface Thermography | Measures the ocular surface temperature and cooling rate during the inter-blink period. | Detects areas of high tear evaporation rate associated with tear film instability. |
Table 1: Table showing non-invasive DED diagnostic techniques and uses. (7,8)
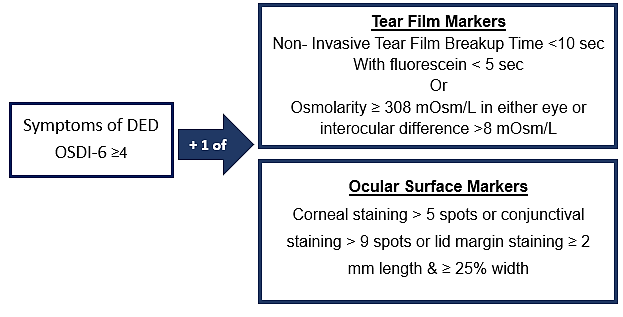

Figure 1: Image showing Diagnostic Criteria for DED
Image Courtesy: Created by the Author
Conclusion
The transition from traditional invasive procedures to non-disruptive diagnostic techniques such as NITBUT, meibography, tear meniscus height evaluation, interferometry and blink rate analysis enables earlier and more accurate detection of DED subtypes, while improving patient comfort. Adopting these techniques supports more precise and consistent results. Beyond clinical precision, non-invasive diagnostics support a patient-focused approach by guiding tailored treatment plans that not only improve ocular health but also enhance comfort, satisfaction, and overall quality of vision.
References
- Nelson, J. D., Craig, J. P., Akpek, E. K., Azar, D. T., Belmonte, C., Bron, A. J., … & Sullivan, D. A. (2017). Tfos dews ii introduction. Ocular Surface, 15(3), 269-275.
- Wolffsohn, J. S., Arita, R., Chalmers, R., Djalilian, A., Dogru, M., Dumbleton, K., … & Craig, J. P. (2017). TFOS DEWS II diagnostic methodology report. The ocular surface, 15(3), 539-574.
- Wang, M. T., Muntz, A., Mamidi, B., Wolffsohn, J. S., & Craig, J. P. (2021). Modifiable lifestyle risk factors for dry eye disease. Contact Lens and Anterior Eye, 44(6), 101409.
- Mehra, D., & Galor, A. (2020). Digital screen use and dry eye: a review. Asia-Pacific journal of ophthalmology, 9(6), 491-497.
- Britten-Jones, A. C., Wang, M. T., Samuels, I., Jennings, C., Stapleton, F., & Craig, J. P. (2024). Epidemiology and risk factors of dry eye disease: considerations for clinical management. Medicina, 60(9), 1458.
- Itokawa, T., Suzuki, T., Koh, S., & Hori, Y. (2023). Evaluating the differences between fluorescein tear break-up time and noninvasive measurement techniques. Eye & Contact Lens, 49(3), 104-109.
- Wolffsohn, J. S., Benítez-Del-Castillo, J., Loya-Garcia, D., Inomata, T., Iyar, G., Liang, L., … & Willcox, M. D. (2025). TFOS DEWS III Diagnostic Methodology. American journal of ophthalmology.
- Pauk, S. V., Petriček, I., Tomić, M., Bulum, T., Jandroković, S., Gulić, M. P., … & Gaćina, D. L. (2023). Diagnostic accuracy of non-invasive tear film break-up time assessed by the simple manual interferometric device. Contact Lens and Anterior Eye, 46(2), 101776.
- Pflugfelder, S. C., Kikukawa, Y., Tanaka, S., & Kosugi, T. (2024). The utility of software-detected non-invasive tear break-up in comparison to fluorescein tear break-up measurements. Frontiers in Medicine, 11, 1351013.
- Tóth, N., Szalai, E., Rák, T., Lillik, V., Nagy, A., & Csutak, A. (2021). Reliability and clinical applicability of a novel tear film imaging tool. Graefe’s Archive for Clinical and Experimental Ophthalmology, 259(7), 1935-1943.
About the Author


Abhirami E
PhD Scholar
SRM Medical College Hospital and Research Centre, Kattankulathur, India