
Vikram B G(1), Bhargavy S(2)
1M.Optom. Student, Dr. Agarwal’s Institute of Optometry, Chennai, India
2Assistant Professor Jr., Dr. Agarwal’s Institute of Optometry, Chennai, India
The global rise in myopia, particularly among children and adolescents, has emerged as a significant public health concern. Myopia not only impairs distance vision but also elevates the long-term risk of serious ocular complications such as glaucoma, cataract, myopic maculopathy, and retinal detachment. In response to this growing burden, myopia control lenses have gained attention as an evidence-based approach to decelerating myopic progression. (1)
Understanding Myopia Control Lenses
Unlike conventional corrective lenses that solely compensate for refractive error, myopia control lenses are specifically engineered to modify the eye’s optical environment and reduce axial elongation, the anatomical hallmark of progressive myopia. These lenses operate by inducing peripheral defocus or reshaping the cornea to alter light distribution across the retina, thereby mitigating signals that drive ocular growth, thereby reducing the progression of myopia. (2)
Types of Myopia Control Lenses
1. Multifocal Contact Lenses
Multifocal lenses are designed with concentric zones or progressive power gradients to correct central vision while simultaneously creating myopic defocus in the peripheral retina. Clinical studies have reported a reduction in myopia progression by approximately 50% when using these lenses. (3)
2. Orthokeratology (Ortho-K)
Rigid-gas-permeable lenses are used as Ortho-K temporarily reshape the cornea when worn overnight, providing clear unaided vision during the day. Ortho-K has demonstrated efficacy in reducing axial elongation beyond refractive correction. Research featured in Optometry and Vision Science indicates a 40–60% reduction in progression among paediatric patients. (4)
3. Myopia Control Spectacle Lenses
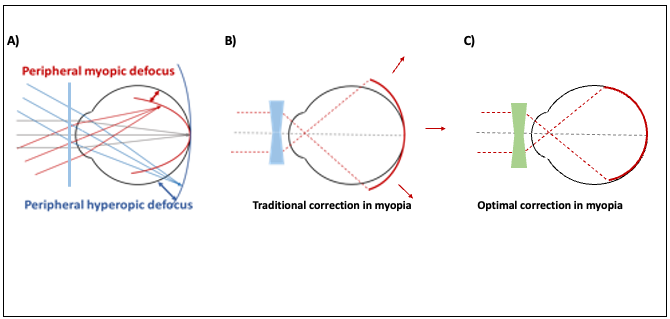
Recent advancements in spectacle lens design with mid-peripheral defocus (Figure 1) offer an effective non-invasive option for myopia control. A longitudinal clinical trial reported a 59% reduction in myopia progression with MiSight lenses over three years. (5)

Figure 1: Depiction of hyperopic defocus and use of myopia control lenses
Efficacy and Clinical Implications
The efficacy of myopia control lenses in slowing the progression of myopia by 40% to 60% is supported by evidence. These interventions do not reverse myopia but serve to manage its trajectory, especially when initiated at an early stage. The therapeutic effect is often enhanced when combined with pharmacological agents such as low-dose atropine eye drops, as supported by findings in recent comparative studies. (6)
Ideal Candidates for Myopia Control Lenses
Myopia control lenses are particularly beneficial for children aged 6 to 18 years who present with mild to moderate myopia and are at risk for rapid progression. A thorough assessment by an eye care professional is essential to tailor the intervention based on refractive status, age, lifestyle, and ocular health. It is mostly beneficial to children with axial myopia. The difference in myopia progression may become obvious at the 18-month or 24-month visit. (7)
Conclusion
As the prevalence of myopia continues to rise, myopia control strategies must become an integral part of paediatric eye care. Myopia control lenses, ranging from multifocal contacts to Ortho-K and DIMS spectacles, offer a viable, clinically validated approach to managing this chronic condition. Early identification, consistent monitoring, and an individualised treatment plan remain pivotal in safeguarding long-term visual outcomes. Though there are newer advancements for myopia control, an effective response can be seen only when these services reach the target population, and they use them. Awareness about these technologies should reach common people, and they should start using them. (1)
References
- Liang, J., Pu, Y., Chen, J., Liu, M., Ouyang, B., Jin, Z., Ge, W., Wu, Z., Yang, X., Qin, C., Wang, C., Huang, S., Jiang, N., Hu, L., Zhang, Y., Gui, Z., Pu, X., Huang, S., & Chen, Y. (2025). Global prevalence, trend and projection of myopia in children and adolescents from 1990 to 2050: a comprehensive systematic review and meta-analysis. The British journal of ophthalmology, 109(3), 362–371. https://doi.org/10.1136/bjo-2024-32542
- Walline, J. J., Jones, L. A., & Sinnott, L. T. (2009). Corneal reshaping and myopia progression. The British journal of ophthalmology, 93(9), 1181–1185. https://doi.org/10.1136/bjo.2008.151365
- Chia, A., Chua, W. H., Wen, L., Fong, A., Goon, Y. Y., & Tan, D. (2014). Atropine for the Treatment of Childhood Myopia: Changes after Stopping Atropine 0.01%, 0.1%, and 0.5%. American Journal of Ophthalmology, 157(2), 451–457.e1. https://doi.org/10.1016/j.ajo.2013.09.020
- Lipson, M. J., Brooks, M. M., & Koffler, B. H. (2018). The Role of Orthokeratology in Myopia Control: A Review. Eye & Contact Lens, 44(4), 224–230. https://doi.org/10.1097/ICL.0000000000000520
- Chamberlain, P., Peixoto-de-Matos, S. C., Logan, N. S., Ngo, C., Jones, D., & Young, G. (2019). A 3-Year Randomized Clinical Trial of MiSight Lenses for Myopia Control. Optometry and Vision Science, 96(8), 556–567. https://doi.org/10.1097/OPX.0000000000001410
- Papadogiannis, P., Börjeson, C., & Lundström, L. (2023). Comparison of Optical Myopia Control Interventions: Effect on Peripheral Image Quality and Vision. Biomedical Optics Express, 14(7), 3125–3137. https://doi.org/10.1364/BOE.486555
- Liu, X., Wang, P., Xie, Z., Sun, M., Chen, M., Wang, J., Huang, J., Chen, S., Chen, Z., Wang, Y., Li, Y., Qu, J., & Mao, X. (2023). One-year myopia control efficacy of cylindrical annular refractive element spectacle lenses. Acta ophthalmologica, 101(6), 651–657. https://doi.org/10.1111/aos.15649
Figure 1: https://forum.wspos.org/wp-content/uploads/2024/10/9.4.png
{kind=link}
Recent Comments