


E. Nivedhitha, M. Optom.
Assistant Professor, Vinayaka Missions Research Foundation, Chennai, India
Zika is an RNA virus that belongs to a family Flaviviridae genus Flavius with well enveloped and inner dense cored with nucleotides and amino acids about 18-45nm size. (1) It was first found in 1947 in Uganda in the rhesus monkey Zika forest, which is how the virus was named Zika. The main vector for Zika virus are mosquitoes of aedes species (A.aegypti and A. albopictus), which lay eggs in fresh water and bite during the daytime. (1)
How Does Zika Spread?
Most people contract the Zika virus through mosquito bites. When a mosquito bites an infected person, it becomes a carrier and can transmit the virus to others nearby spreading rapidly within communities. Other transmission routes include mother-to-fetus transmission during pregnancy, sexual contact, and blood transfusion. (1,2)
Symptoms
Zika virus infection often presents with the following symptoms:
- Headache
- Fever
- Joint pain
- Muscle pain
- Conjunctivitis
- Rashes
Symptoms typically appear 2–14 days after the bite and usually last several days to a week. (2)
Zika Virus Association with Microcephaly
The major concern associated with Zika infection is the apparent increased incidence of microcephaly in fetuses born to mothers infected with ZIKA. When pregnant women are affected, pass the Zika virus to the fetus during pregnancy. (3)
Zika causes microcephaly, a condition in which the baby’s head is relatively smaller than expected due to abnormal brain development. Zika interferes with the normal process of neurogenesis by primarily targeting the neural progenitor cells (NPC cells), which are responsible for generating neurons, causing them to die and premature differentiation that leads to reduced neurons. This reduced number of neurons will end up with many abnormal brain developments, including microcephaly. (3)
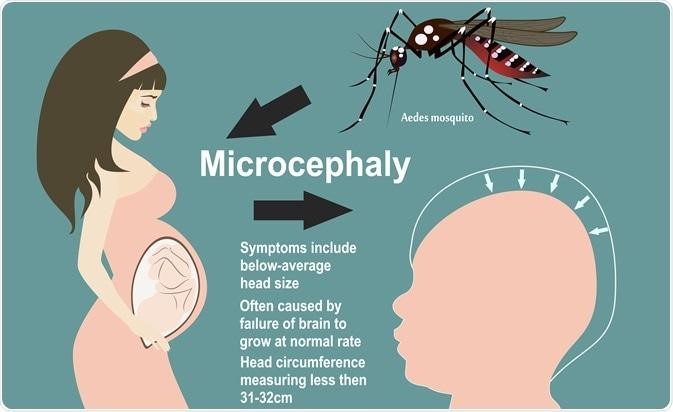

Figure 1: Microcephaly due to Zika virus-infected mother
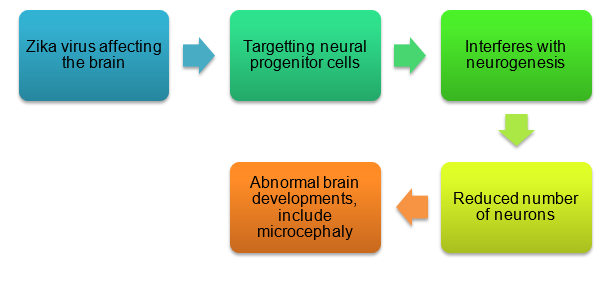
Figure 2: Pathophysiology of Microcephaly due to Zika Virus
Congenital Zika Syndrome (CZS)
Is a pattern of birth defects in babies infected with Zika during pregnancy.
- Small head size (microcephaly)
- Brain damage
- Seizures
- Hearing and vision problems
- Motor and limb movement difficulties
- Feeding challenges (difficulty swallowing) (4)
Prenatal Influences on Vision Development by Zika
The Zika virus can directly harm retinal tissue and cause inflammation by piercing the blood retinal barrier and entering the eye, leading to visual problem.
This can result in adult infections that cause anterior uveitis and non purulent conjunctivitis. The virus can harm Muller glial cells, ganglion cells, and retinal pigmented epithelium cells in newborns with congenital Zika syndrome (CZS). (5,6)
Congenital Zika syndrome is presented with these ocular findings
- Optic nerve hypoplasia
- Chorioretinal atrophy
- Iris coloboma
- Night blindness
- Tunnel vision
- Retinal pigment epithelial mottling
- Torpedo maculopathy
- Haemorrhagic maculopathy (5,6)
Diagnosis
Zika infection is diagnosed using laboratory tests that detect viral genetic material (RT-PCR) or antibodies (serology), commonly from blood or urine samples. (2)
Treatment and Prevention
Currently, there is no cure or direct treatment for Zika virus-related visual problems. It is important to stay away from mosquito bites and have protected intercourse to avoid getting virus in the first phase. Dilated eye examination and other eye tests within the month of delivery can identify visual problems in newborns who have been exposed during pregnancy. This enables early access to low vision care and early intervention to improve the child’s visual and developmental potential. (2,5)
Conclusion
People infected with the Zika virus should drink enough fluids, get plenty of rest and treat pain and fever with common medicines. If symptoms worsen, they should seek immediate medical attention. Prevention is always better than cure; one should prevent mosquito bites as much as possible. (2)
References
- Noorbakhsh F, Abdolmohammadi K, et al. Zika Virus Infection, Basic and Clinical Aspects: A Review Article. Iran J Public Health. 2019;48(1):20–31. PMID: 30847308; PMCID: PMC6401583.
- Plourde AR, Bloch EM. A Literature Review of Zika Virus. Emerg Infect Dis. 2016;22(7):1185–1192. doi:10.3201/eid2207.151990.
- Gharbaran R, Somenarain L. Putative Cellular and Molecular Roles of Zika Virus in Fetal and Pediatric Neuropathologies. Pediatr Dev Pathol. 2019;22(1):5–21.
- Kuadkitkan A, et al. Zika Virus and Microcephaly in Southeast Asia: A Cause for Concern? J Infect Public Health. 2020;13(1):11–15.
- Heymann DL, Hodgson A, Sall AA, et al. Zika Virus and Microcephaly: Why Is This Situation a PHEIC? Lancet. 2016;387(10020):719–721.
- Tan JJL, Balne PK, Leo YS, Tong L, Ng LFP, Agrawal R. Persistence of Zika Virus in Conjunctival Fluid of Convalescent Patients. 2017.
- Labib BA, Chigbu DI. Pathogenesis and Manifestations of Zika Virus-Associated Ocular Diseases. Trop Med Infect Dis. 2022;7:106.
- Agence France-Presse. Spain Reports First Known European Case of Zika-Infected Pregnant Woman. The Guardian. Feb 4, 2016.
- Mathur N. Study Reveals the Inevitability of Zika Virus Dumbbell-1 Structure for Viral Pathogenesis. News-Medical. May 17, 2023.