Varsha Singh, M. Optom
Assistant Professor, KD Institute of Allied Health Sciences, Ahmedabad, India
The term “Akinetopsia” was coined by Zeki in 1991, which is also called “motion blindness”. (1) It features a complete lack or severe reduction in the ability to perceive smooth object motion where instead moving items appear as static snapshots or freeze-frames that suddenly leap between spots much like the flashing effect of a stroboscope. (2,3)
Visual motion perception is vital for more than just basic detection; impairments in it severely impair everyday activities such as walking, navigating public transport, viewing television, reading, interacting socially, and preparing meals frequently making these tasks challenging or unfeasible. (4-7) This capability is furthermore vital for safety and survival across numerous situations, encompassing depth perception, travel, athletics, and common activities like grasping objects or extending for items. It underpins nonverbal cues as well, including interpreting gestures, posture, and lip-reading. (2,4-8)
Pathway of Motion Processing
The perception of motion begins in the retina, where parasol ganglion cells detect movement and low-contrast cues and transmit signals to the Lateral Geniculate Nucleus (LGN), which contains motion-sensitive magnocellular layers for rapid transmission. From the LGN, signals reach the primary Visual Cortex (V1), specifically layer 4Cα and then layer 4B, where direction-selective neurons detect initial motion. Following this, the signals are transmitted to secondary visual areas, including V2 (thick stripes) and V3, where motion is integrated with depth. Finally, the signals reach the V5/MT region, where speed, direction, and complex motion patterns are detected. This entire pathway contributes to the perception of motion and spatial awareness. Thus, motion blindness arises from damage to the magnocellular pathway, specifically the V5/MT area, leading to an inability to perceive motion.
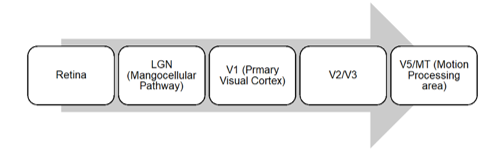
Figure 1: This image shows the pathway of motion perception.
Image Courtesy: Created by the Author
Types of Akinetopsia
Akinetopsia is broadly classified into two types: Gross and Fine.
| Type | Description | Clinical Features | Lesion Site |
|---|---|---|---|
| Gross Akinetopsia | Complete loss of motion perception | Sees objects as static frames, cannot detect movement | Usually bilateral V5/MT damage |
| Fine Akinetopsia | Partial/subtle impairment of motion perception | Motion seen but impaired, poor speed and direction judgment | Partial damage to V5/MT or dorsal pathway |
Table 1: This table shows the clinical features of different types of Akinetopsia.
Diagnostic Procedures
Without standardised diagnostic tools, Akinetopsia assessments typically involve a comprehensive history, full physical exams (general, ophthalmic, neurologic, and psych/psychiatric), blood tests, and supportive imaging like brain Computed Tomography/Magnetic Resonance Imaging (CT/MRI), Electroencephalogram (EEG), plus psychophysical evaluations. These often cover eye tracking, motion-direction identification, contrast sensitivity to drifting gratings, random dot kinematograms, speed discrimination, and motion-defined form tasks. (11-13)
Management
Current primary treatments for Akinetopsia rely on practical approaches that target either the root cause (typically via medications) or its downstream impacts. (10)
For instance, certain research suggests rehabilitation potential via targeted training to restore intact elements of visual motion processing. Several cases show patients unaware of their motion perception deficit until it caused phobias or crashes, revealing common unawareness and its dangers, deeper insights into Akinetopsia can elevate awareness in science clinics and society, urging tailored support systems for its challenges, prioritising quality-of-life gains fosters inclusion, clinically prioritise full workups, treat underlying issues, motion rehab training, and psychoeducation. (10)
Conclusion
Akinetopsia is a condition where a person cannot perceive motion, which is due to damage to the magnocellular pathway, especially the V5/MT area, which has several causes and affects the daily life activities of a person and can even lead to death. (1-7) Detailed medical history, along with brain imaging techniques, helps in its diagnosis and in finding the root cause. (11-13) Currently, for its management, rehabilitation, counselling, and psychoeducation are suggested, and other treatment options are also under trial. (10)
References
- Zeki, S. (1991). Cerebral akinetopsia (visual motion blindness) a review. Brain, 114(2), 811-824.
- Barton, J. J. (2011). Disorders of higher visual processing. Handbook of clinical neurology, 102, 223-261.
- Burns, M. S. (2004). Clinical management of agnosia. Topics in stroke rehabilitation, 11(1), 1-9.
- Zihl, J., von Cramon, D., & Mai, N. (1983). Selective disturbance of movement vision after bilateral brain damage. Brain: A Journal of Neurology, 106 (Pt 2)(2), 313–340.
- Campbell, R., Zihl, J., Massaro, D., Munhall, K., & Cohen, M. M. (1997). Speechreading in the akinetopsic patient, LM. Brain: a journal of neurology, 120(10), 1793-1803.
- Pelak, V. S., & Hoyt, W. F. (2005). Symptoms of akinetopsia associated with traumatic brain injury and Alzheimer’s disease. Neuro-Ophthalmology, 29(4), 137-142.
- Zihl, J., & Heywood, C. A. (2015). The contribution of LM to the neuroscience of movement vision. Frontiers in Integrative Neuroscience, 9, 6.
- Huberle, E., Rupek, P., Lappe, M., & Karnath, H. O. (2012). Perception of biological motion in visual agnosia. Frontiers in behavioral neuroscience, 6, 56.
- Newsome, W. T., & Pare, E. B. (1988). A selective impairment of motion perception following lesions of the middle temporal visual area (MT). Journal of Neuroscience, 8(6), 2201-2211.
- Browne, J. L., Krabbendam, L., & Blom, J. D. (2025). Akinetopsia: a systematic review on visual motion blindness. Frontiers in Neurology, 15, 1510807.
- Becker, H. G., Haarmeier, T., Tatagiba, M., & Gharabaghi, A. (2013). Electrical stimulation of the human homolog of the medial superior temporal area induces visual motion blindness. Journal of Neuroscience, 33(46), 18288-18297.
- Maeda, K. (2019). Akinetopsia on driving. Journal of stroke and cerebrovascular diseases, 28(7), e102-e103.
- Shipp, S., Jong, B. D., Zihl, J., Frackowiak, R. S. J., & Zeki, S. (1994). The brain activity related to residual motion vision in a patient with bilateral lesions of V5. Brain, 117(5), 1023-1038.
About the Author

Varsha Singh
Assistant Professor
Recent Comments