Dr. Alex Ong, DOptom, FAAO, FOWNS, CPNP (US)
Managing Director and Optometrist, Ong’s Optics Myopia Management Centre
Introduction
Myopia is increasingly understood as a structural ocular condition involving axial elongation and posterior pole remodelling. Beyond refractive error, progressive Myopia is associated with choroidal thinning and altered ocular perfusion. Choroidal thickness (ChT) has emerged as an important structural biomarker in Myopia and is strongly associated with Myopic Maculopathy and long-term visual impairment risk.(1,2)
Macular pigment optical density (MPOD), reflecting retinal lutein, zeaxanthin, and meso-zeaxanthin concentrations, plays a protective role via antioxidant and anti-inflammatory mechanisms. Although widely studied in Age-related Macular Degeneration, emerging evidence suggests MPOD may also be relevant in paediatric ocular development and Myopia.
This case report describes a Myopic child presenting with both reduced MPOD and markedly thin choroid and explores potential mechanistic and clinical implications.
Case Presentation
An 11-year-old child with bilateral Myopia underwent comprehensive examination. He has been Myopic since age of 9 year-old. Single vision lenses was prescribed to him by the practitioner with SE of -1.50 D both eyes.
As there was a significant increase in his Myopia one year ago, with a -1.50 D increase both eyes, he has been wearing Highly Aspheric Lenslet Target (HALT) defocus lenses of SE -3.00D OU. Myopia progressed about -0.75D within a year for OU and parents wanted a second opinion and visited our practice.
During the visit, axial length was measured and it was 25.60mm for the OD and 25.56mm for the OS.
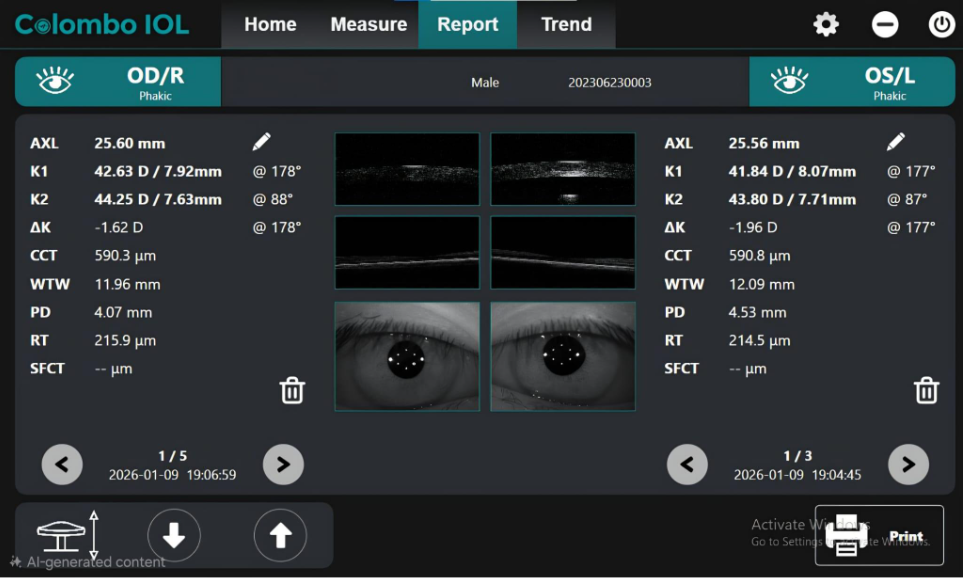
Figure 1: This image shows axial length measurement of both eyes using Colombo OCT Biometer.
Image Courtesy: Captured by Author
Using a SD-OCT build in the biometer, it was found that his ChT was quite thin, with OD having a ChT of 213 µm and OS having 195 µm.
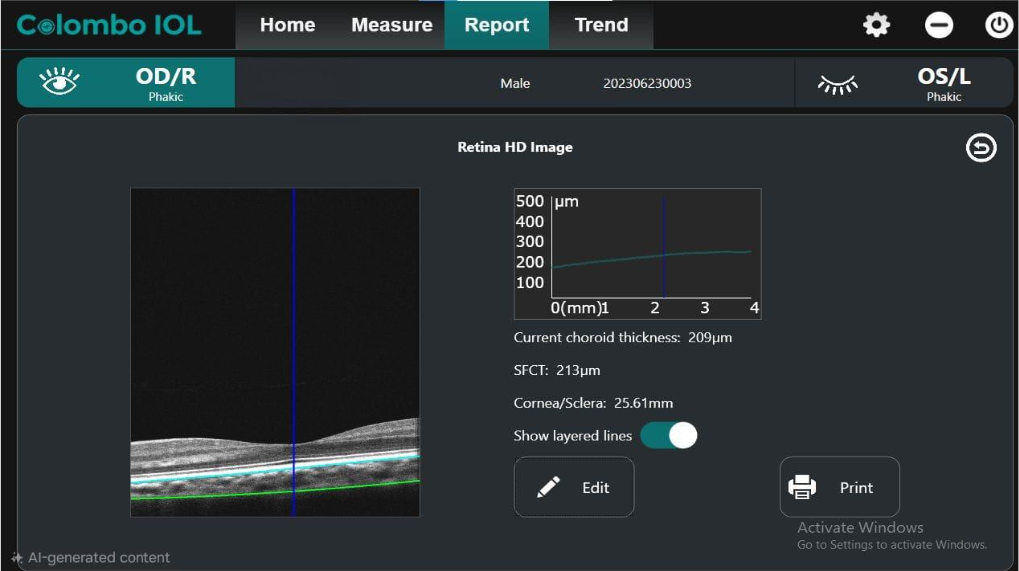
Figure 2: This image shows ChT measurement of the Right Eye (213μm) using Colombo OCT Biometer.
Image Courtesy: Captured by Author
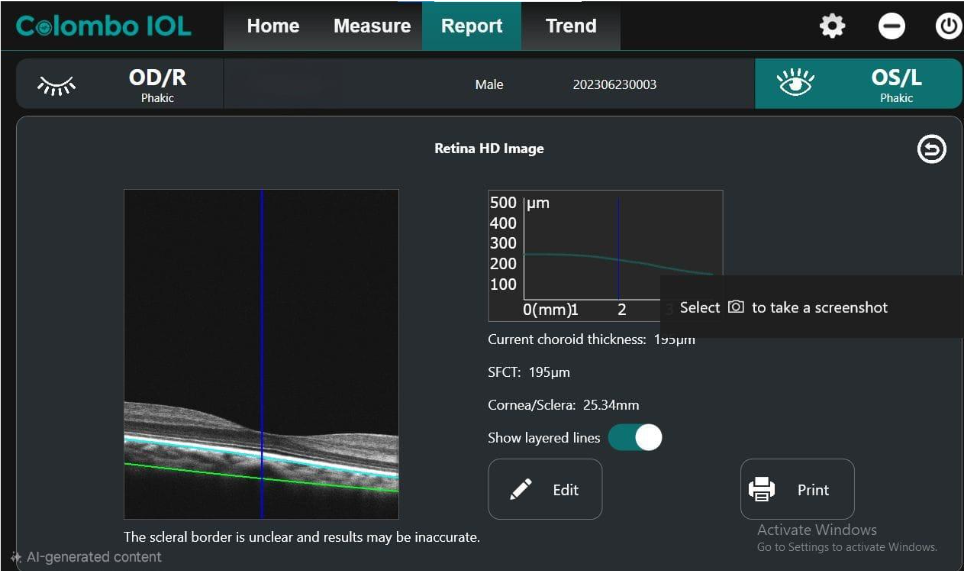
Figure 3: This image shows ChT measurement of the Left Eye (195μm) using Colombo OCT Biometer.
Image Courtesy: Captured by Author
An MPOD test using the heterochromatic flicker photometry revealed the following result:
- OD: 0.48
- OS: 0.38
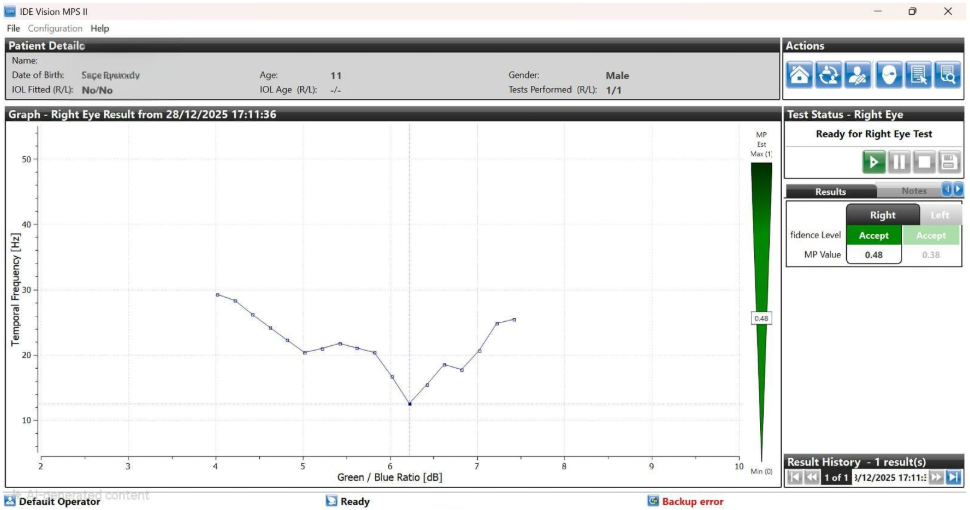
Figure 4: This image shows result from MPSII MPOD testing showing Right and Left eyes MPOD value.
Image Courtesy: Captured by Author
No clinical evidence of Myopic Maculopathy was observed at presentation.
DiscussionMyopia management has traditionally focused on refractive error progression and axial length elongation as primary outcome measures. While these parameters remain clinically important, they may not fully capture the overall structural and physiological health of the eye. Increasingly, attention has turned toward posterior segment changes, particularly the choroid, as an integral component of Myopia pathophysiology. In some children, reliance on refractive and axial metrics alone may overlook underlying structural vulnerability.
In the present case, the child demonstrated a refractive progression of approximately −0.75 D per year, which would generally be considered a moderated rate of progression with the use of peripheral defocus lenses. Axial length remained below 26 mm, a threshold often associated with higher risk of pathological Myopia. However, despite these seemingly favourable indicators, subfoveal ChT was measured at approximately 190–210 µm, which is substantially thinner than expected for age. This discrepancy raises the question of whether current Myopia management strategies may underestimate risk in children who exhibit relatively controlled refractive progression but possess underlying choroidal thinning and potential vascular compromise.
Choroidal Thinning in Paediatric Myopia
Understanding normative ChT in children is essential before interpreting pathological changes. In a large paediatric cohort of healthy children aged 4–12 years with minimal refractive error, the mean subfoveal ChT was reported to be approximately 330 ± 65 µm, with values ranging from 189 to 538 µm. (3) Importantly, ChT was found to increase with age during childhood, suggesting that a relatively thick and well-perfused choroid is a normal feature of ocular development. (3) Other paediatric studies have similarly demonstrated that ChT is influenced by age, axial length, and refractive status, with thicker choroids generally observed in emmetropic or low Myopic eyes. (3,4) These findings provide an important baseline reference for distinguishing physiological variation from early structural abnormalities.
When considering ethnicity-specific data, studies in East Asian populations, particularly Chinese children, report slightly lower mean subfoveal ChT values of approximately 302 ± 63 µm in children aged 6–12 years. (5) Given the higher prevalence and earlier onset of Myopia in Asian populations, these values are particularly relevant for clinical interpretation in the present case.
In contrast to normative populations, children with Myopia consistently demonstrate thinner choroids compared to non-Myopic peers, and this thinning becomes more pronounced with increasing axial length and Myopia severity.(4,6) Longitudinal evidence further supports this relationship. In a 4-year cohort study of Myopic children, choroidal thickness remained relatively stable during early, moderate Myopia but showed significant thinning as Myopia progressed to higher levels, particularly in children with greater refractive progression. (4) These findings suggest that choroidal thinning is not only associated with Myopia but may also reflect disease progression and structural remodelling over time.
In addition, systematic evidence indicates that ChT is a dynamic and responsive biomarker, capable of changing in response to optical and pharmacological interventions, and may act as both an indicator and mediator of Myopia progression. (7) Choroidal thinning has been linked to hyperopic defocus and axial elongation, while choroidal thickening is observed with effective Myopia control strategies, further supporting its functional role in ocular growth regulation. (7)
In the present case, the measured subfoveal ChT of approximately 190–210 µm is substantially below both global paediatric norms (~330 µm) and Asian-specific values (~300 µm). This places the child within a relatively thin-choroid phenotype for age. Given that choroidal thinning is associated with axial elongation, reduced ocular blood flow, and increased risk of Myopic Macular Degeneration, this finding raises important clinical considerations that extend beyond refractive error and axial length alone. (1,2,6)
Thus, choroidal thickness should be interpreted not only as a structural correlate of Myopia but also as a potential biomarker of posterior pole health and long-term ocular risk.
MPOD in Paediatric Myopia
With such a presentation, macular pigment optical density (MPOD) represents an additional parameter reflecting the biochemical and vascular status of the posterior pole. MPOD values in school-aged Chinese children average approximately 0.56 ± 0.25, (8) and the present child’s values (0.48 OD / 0.38 OS) lie within reported ranges but trend toward the lower end.
Current evidence does not demonstrate a consistent direct relationship between MPOD and structural parameters such as choroidal thickness, particularly in paediatric populations.(8) However, studies suggest that increasing Myopic refractive error may be associated with reduced MPOD, indicating altered retinal carotenoid status in Myopic eyes.(9)
Macular pigment, composed of lutein, zeaxanthin, and meso-zeaxanthin, plays a key role in antioxidant protection and maintenance of retinal integrity. (10) Reduced MPOD may therefore reflect diminished oxidative buffering capacity in the posterior pole. While MPOD and choroidal thickness may not be directly correlated, they may share common underlying pathways related to vascular regulation and oxidative stress. Supporting this, carotenoid supplementation has been shown to improve ocular blood flow, (11) and in paediatric populations, lutein supplementation has been associated with attenuation of choroidal thinning. (12)
Taken together, the relatively lower MPOD observed in this case, alongside reduced choroidal thickness, may reflect a broader ocular environment characterised by reduced antioxidant capacity and compromised vascular support, rather than a direct causal relationship between the two parameters.
Linking MPOD, Choroidal Perfusion, and Axial Elongation
A biologically plausible pathway may connect low MPOD and reduced ChT: choroidal perfusion is essential for metabolic support of the outer retina and sclera. Reduced oxygen delivery may stimulate matrix metalloproteinase activity and extracellular matrix remodelling, reducing scleral rigidity and facilitating globe elongation.
While causality cannot be established in this case, the coexistence of reduced MPOD and markedly thin choroidal thickness may reflect a state of impaired oxidative and vascular support within the posterior pole. Previous studies have demonstrated associations between lower MPOD and reduced choroidal structural and vascular parameters, as well as decreased choriocapillaris perfusion in Myopic and retinal disease conditions. (11,13) This supports the possibility that such findings may represent a vascular–oxidative susceptibility profile in paediatric Myopia.
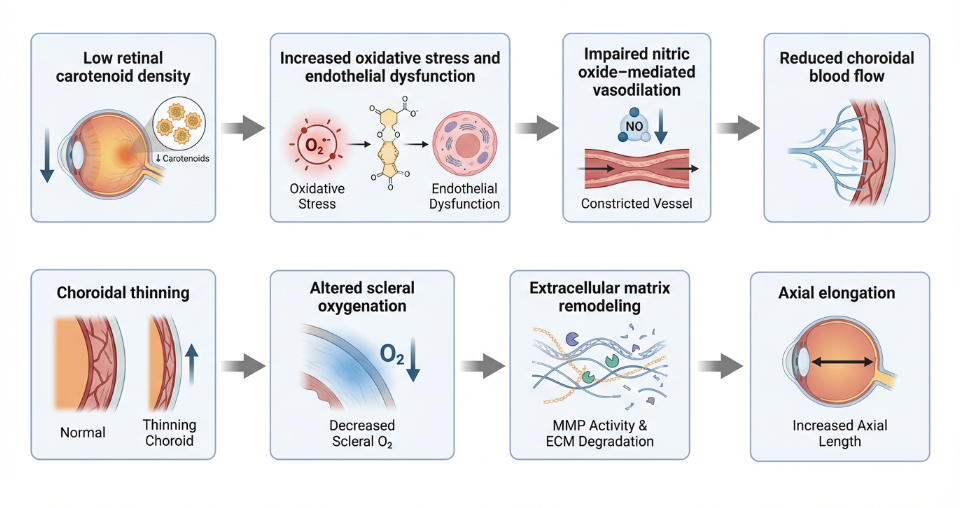
Figure 5: This diagram shows an illustration of the link between MPOD, Choroidal Perfusion and possible Axial Elongation theory.
Image Courtesy: Captured by Author
While Myopia management has largely focused on reducing refractive progression and limiting axial elongation to prevent future complications, this case highlights a potential gap in current approaches. Despite relatively controlled refractive progression and axial length within lower-risk ranges, the presence of reduced MPOD and markedly thin choroidal thickness suggests that the underlying ocular environment may not be fully optimised.
The choroid plays a critical role in supplying oxygen and nutrients to the outer retina and sclera, as well as facilitating metabolic waste removal. Reduced choroidal thickness may therefore reflect compromised vascular and metabolic support within the posterior segment. In this context, focusing solely on refractive and axial metrics may overlook important aspects of retinal health.
This observation suggests that Myopia management should extend beyond slowing progression to include preservation of retinal integrity, vascular function, and overall ocular health. Parameters such as MPOD and choroidal thickness may provide additional insight into the biological environment of the eye and highlight the need for adjunctive strategies targeting oxidative balance and choroidal perfusion.
Therefore, beyond optical and pharmacological interventions, what additional strategies can Optometrists adopt to support children presenting with such underlying structural and biochemical vulnerabilities?
Nutritional Modulation of Choroidal Structure and Perfusion
Emerging evidence suggests carotenoid supplementation can influence choroidal metrics.
-
Lutein
A randomised controlled trial in children aged 8–12 years demonstrated that 6 months of lutein ester supplementation significantly mitigated subfoveal and temporal choroidal thinning compared with placebo. (12) Although axial length changes were not significant over the short duration, stabilisation of ChT suggests early structural modulation. In adult supplementation data, it was demonstrated that lutein complex increases ocular blood flow biomarkers, supporting vascular mechanisms.(11)
-
Crocetin
A paediatric randomised clinical trial demonstrated that crocetin supplementation reduced Myopia progression and axial elongation. (14) Proposed mechanisms include nitric oxide–mediated vasodilation and improved choroidal perfusion.
-
Astaxanthin
Astaxanthin supplementation significantly increased choroidal blood flow velocity in controlled human trials. (15) Combination antioxidant supplementation has also been shown to improve choroidal structural parameters in adult retinal disease cohorts.(16) Although extrapolation to paediatric Myopia requires caution, these findings demonstrate that choroidal perfusion and thickness are modifiable.
Taken together, these findings suggest that nutritional support, particularly through carotenoid supplementation, may play an important adjunctive role in modulating choroidal structure and perfusion. While optical and pharmacological interventions remain the cornerstone of Myopia management, emerging evidence indicates that strategies targeting oxidative balance and vascular function may contribute to maintaining posterior pole health. Therefore, incorporating evidence-based nutritional support may represent a valuable component of a more comprehensive and holistic approach to Myopia management in children.
However, an important part to note that, this report is limited to a single case, and MPOD measurements in children may be influenced by fixation stability and methodological variability. Furthermore, a direct causal relationship between MPOD and choroidal thickness cannot be established based on current evidence. Larger longitudinal paediatric studies are required to better elucidate the interactions between macular pigment, choroidal structure, and Myopia progression, as well as to determine the long-term impact of nutritional interventions on ocular health.
Conclusion
The coexistence of reduced MPOD and markedly thin choroidal thickness in this Myopic child suggests a potential vascular–oxidative susceptibility profile within paediatric Myopia. Given the established association between choroidal thinning and increased risk of Myopic Macular Degeneration, evaluation of posterior pole structure and biochemical status may provide additional insight beyond conventional refractive error and axial length measurements. These findings indicate that structural and functional metrics of the eye should be considered as part of a more comprehensive assessment of Myopia risk.
Accordingly, Myopia management may need to evolve beyond a predominantly refractive-centred approach toward one that incorporates overall ocular health. Optometrists play an important role not only in slowing Myopia progression through optical and pharmacological interventions, but also in monitoring structural integrity and supporting retinal and choroidal health. Such an integrated approach may improve long-term visual outcomes, although further longitudinal studies are required to validate these associations.
References
- Liu R, Xuan M, Wang DC, Xiao O, Guo XX, Zhang J, et al. Using choroidal thickness to detect myopic macular degeneration. Int J Ophthalmol. 2024;17(2):317–323.
- Ueda E, Yasuda M, Fujiwara K, Hashimoto S, Honda T, Nakamura S, et al. Association between choroidal thickness and myopic maculopathy in a Japanese population: the Hisayama Study. Ophthalmol Sci. 2023;3(4):100350. doi:10.1016/j.xops.2023.100350.
- Read SA, Collins MJ, Vincent SJ, Alonso-Caneiro D. Choroidal thickness in childhood. Invest Ophthalmol Vis Sci. 2013;54(5):3586–3593.
- Lee JH, Shin JY, Kim M, Lee KM, Oh S, Kim SH, et al. Changes in choroidal thickness of healthy children during myopia progression over 4 years: Boramae Myopia Cohort Study Report 5. Ophthalmol Sci. 2024;5:100688.
- He X, Jin P, Zou H, Li Q, Jin J, Lu L, et al. Choroidal thickness in healthy Chinese children aged 6 to 12 years: The Shanghai Children Eye Study. Retina. 2017;37(2):368–375.
- Yang YS, Koh JW. Choroidal blood flow change in eyes with high myopia. Korean J Ophthalmol. 2015;29(5):309–314.
- Martinez-Perez C, Oliveira AP. Impact of myopia control interventions on choroidal thickness in children: a systematic review and meta-analysis of randomized controlled trials. Ophthalmol Sci. 2025;6(2):101039.
- Zheng W, Zhang Z, Jiang K, Zhu J, He G, Ke B. Macular pigment optical density and its relationship with refractive status and foveal thickness in Chinese school-aged children. Curr Eye Res. 2013;38(1):168–173.
- Tong N, Zhang Z, Wang Q, Wu Y, Liu Y, Zhang X. Inverse relationship between macular pigment optical density and axial length in Chinese subjects with myopia. Invest Ophthalmol Vis Sci. 2013;251(6):1495–1500.
- Ponce-García V, et al. Analysis of macular pigment optical density in childhood: a systematic review. Surv Ophthalmol. 2024;39(8):577–585.
- Harris A, Siesky B, Huang A, Do T, Mathew S, Frantz R, et al. Lutein complex supplementation increases ocular blood flow biomarkers in healthy subjects. Int J Vitam Nutr Res. 2019;89(1–2):5–12.
- Li T, et al. Effect of lutein ester supplementation on choroidal thickness in children: a randomized controlled trial. 2025;14(12):1–14.
- Ruggeri ML, Belloni Baroni L, Passamonti M, Quarta A, Lorenzi C, Formenti F, et al. OCT analysis and macular pigment optical density assessment in patients affected by retinitis pigmentosa. Sci Rep. 2024;14:28830.
- Mori K, Kurihara T, Miyake Y, et al. The effect of dietary supplementation of crocetin for myopia control in children: a randomized clinical trial. Sci Rep. 2019;8(8):1179:1–14.
- Saito M, Yoshida K, Saito W, Fujiya A, Ohgami K, Kitaichi N, et al. Astaxanthin increases choroidal blood flow velocity. Graefes Arch Clin Exp Ophthalmol. 2012;250(2):239–245.
- D’Aloisio R, Di Antonio L, Toto L, Rispoli M, Di Iorio A, Delvecchio G, et al. Choroidal changes in blood flow in patients with intermediate age-related macular degeneration after oral dietary supplementation. Medicina (Kaunas). 2022;58(8):1092.
About the Author

Dr. Alex Ong, DOptom, FAAO, FOWNS, CPNP (US)
Optometrist, Singapore
PGCert (Anterior Eye Diseases, Cataract and Glaucoma)
PGCert (Retinal Disease Recognition and Co-Management)
MSCO, B.Sc Optom, Dip. Optom
Dr. Ong is the Founder and Managing Director/Optometrist at Ong’s Optics Myopia Management Centre, established in 2005 and 2nd generation owner of Ong’s Optics and Contact Lens Centre, established in 1985. With over two decades of clinical experience, his expertise spans evidence-based Myopia management, ocular nutrition, binocular vision, orthokeratology, and geriatric vision care. He serves as a Key Opinion Leader for Menicon Japan and has taught as an adjunct lecturer at both Optometry schools in Singapore. Dr. Ong is actively involved in Optometric education and professional training across Asia. As a Certified Personalised Nutrition Practitioner (CPNP) with the American Nutrition Association, he integrates nutritional science with vision care to promote a proactive and preventive model of lifelong eye health. He is also a member and Fellows of Ocular Wellness and Nutrition Society.
Recent Comments