Saptarshi Mukherjee, M. Optom, F. Optom
Senior Optometrist, Centre for Sight New Delhi, India
Introduction
Glaucoma remains a leading cause of irreversible blindness worldwide, and trabeculectomy continues to be one of the most commonly performed surgical procedures for lowering intraocular pressure (IOP) when medical and laser therapies are insufficient. However, surgical success is not determined solely by post-operative IOP measurements. A key determinant of long-term outcome is filtering bleb function, which refers to the performance of the subconjunctival reservoir created during surgery to facilitate aqueous humour outflow from the anterior chamber.
To standardise bleb evaluation and improve communication among clinicians and researchers, several grading systems have been developed. These systems enable structured assessment of bleb morphology, support prediction of long-term surgical success, and assist in guiding post-operative management, particularly in decisions regarding interventions such as needling, antimetabolite therapy, or surgical revision.
This review summarises the rationale for bleb grading, describes the major grading systems currently in use, and discusses their strengths, limitations, and relevance in contemporary Glaucoma practice.
Why Grade a Bleb?
Not all filtering blebs are equivalent in morphology or function. Bleb characteristics such as elevation, vascularity, cystic changes, and flattening reflect underlying differences in aqueous humour filtration and are closely associated with surgical outcomes and prognosis.
Functional Blebs: Functional blebs typically appear diffuse, moderately elevated, and avascular with a healthy surrounding conjunctiva.
Nonfunctional Blebs: Nonfunctional blebs may be flat, encapsulated, or show excessive vascularity, leading to inadequate IOP control.
Dangerous Blebs: Dangerous blebs (e.g., thin, avascular, leaking blebs) predispose to hypotony, blebitis, or endophthalmitis.
Structured grading of bleb morphology enables clinicians to:
- Longitudinally assess morphological changes over time.
- Estimate the probability of surgical success or failure.
- Facilitate comparison of outcomes across studies and populations.
- Promote standardised reporting in clinical trials.
Evolution of Bleb Grading
Prior to the 1990s, evaluation of filtering blebs was predominantly qualitative and lacked standardisation, with clinicians relying on descriptive terms such as “diffuse,” “flat,” or “vascular.” The need for objective and reproducible assessment subsequently led to the development of structured grading systems incorporating slit-lamp biomicroscopy and standardised photographic references.
Over time, multiple systems emerged, each with a unique focus, some emphasised bleb height and extent, others vascularity, and still others added features such as leakage or internal reflectivity with anterior segment imaging.
1. Würzburg Bleb Classification System
Represents one of the early structured approaches to bleb assessment, developed to standardise post-operative evaluation following Glaucoma filtration surgery.
Parameters
- Vascularity
- Encapsulation
- Presence of microcysts
- Bleb morphology (diffuse vs localised)
Scale
Each parameter is graded using a categorical scoring system
based on slit-lamp biomicroscopy.
Strengths
- Provides a more structured morphological assessment compared to purely descriptive methods.
- Clinically applicable and relatively straightforward to use.
Weaknesses
- Limited standardisation due to lack of widely adopted photographic reference scales.
- Potential for interobserver variability.
WBCS contributed to the evolution of bleb evaluation by introducing structured morphological criteria, paving the way for later grading systems incorporating standardised photographic references and improved reproducibility.
2. Indiana Bleb Appearance Grading Scale (IBAGS)
Published in 2003, the Indiana Bleb Appearance Grading Scale (IBAGS) became one of the most widely adopted systems for standardised assessment of filtering blebs in clinical research. It utilises slit-lamp biomicroscopy supported by photographic reference standards to improve grading consistency.
Parameters
- Height (H0–H3): Flat to highly elevated
- Extent (E0–E3): Graded based on circumferential limbal involvement
- Vascularity (V0–V4): Ranging from avascular to highly vascular
- Seidel test (S0–S2): Absence or presence of leakage
Advantages
- Incorporates standardised photographic references, enhancing reproducibility.
- Relatively simple and applicable in both clinical and research settings.
- Widely used in multicentre studies.
Limitations
- Primarily evaluates external bleb morphology without assessing internal structure.
- Subject to moderate interobserver variability.
IBAGS represented a significant advancement in bleb assessment by improving standardisation and reproducibility, particularly in multicentre glaucoma trials.
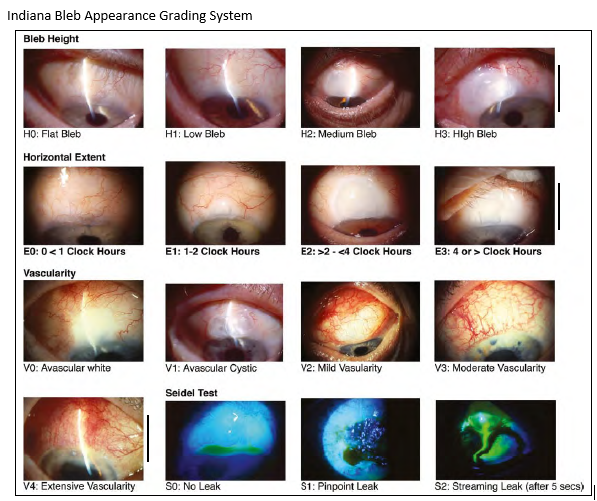
Figure 1: This image shows the Indiana Bleb Appearance grading system. (2)
3. Moorfields Bleb Grading System (MBGS)
Developed at Moorfields Eye Hospital, the Moorfields Bleb Grading System (MBGS) is one of the most widely used and reproducible systems for standardised assessment of filtering blebs. It incorporates slit-lamp evaluation supported by standardised photographic references to enhance grading consistency.
Parameters
- Area (A): Extent of the bleb relative to the limbus, graded using reference photographs
- Height (H): Graded from low to high elevation
- Vascularity (V): Assessed separately for the central bleb and peripheral bleb regions
- Seidel test (S): Recorded separately to indicate the presence or absence of leakage
Advantages
- A comprehensive photographic reference library enhances interobserver agreement and grading reproducibility.
- Separate assessment of central and peripheral vascularity enables more nuanced evaluation of bleb perfusion.
- Widely used in clinical trials and research settings.
Limitations
- More time-consuming to apply compared with IBAGS.
- Requires training and experience to achieve consistent grading.
MBGS represents a refinement over earlier systems by combining structured grading with photographic references, improving interobserver agreement and facilitating standardised reporting in clinical studies.
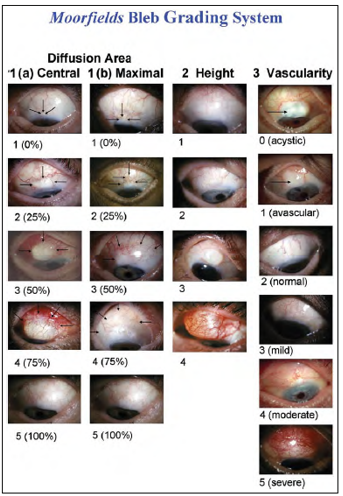
Figure 2: This image shows the Moorfield Bleb grading systems appearance. (4)
Advanced Imaging-Based Grading Systems
With the advent of anterior segment optical coherence tomography (AS-OCT) and ultrasound biomicroscopy, imaging-based approaches to bleb assessment have gained prominence. The long-term success of glaucoma filtration surgery largely depends on the functional integrity of the filtering bleb, a subconjunctival reservoir created intraoperatively to facilitate aqueous humour drainage from the anterior chamber into the subconjunctival space. These imaging modalities provide detailed structural information that cannot be appreciated on conventional slit-lamp examination, including:
- Internal bleb cavities
- Subconjunctival fluid distribution
- Encapsulation and fibrotic changes
- Scleral flap configuration and morphology
Although these imaging techniques have not yet been incorporated into a universally standardised grading system, they are increasingly utilised in research settings and offer objective, quantitative insights. As such, they are likely to complement and potentially enhance traditional slit-lamp based grading systems in the future.
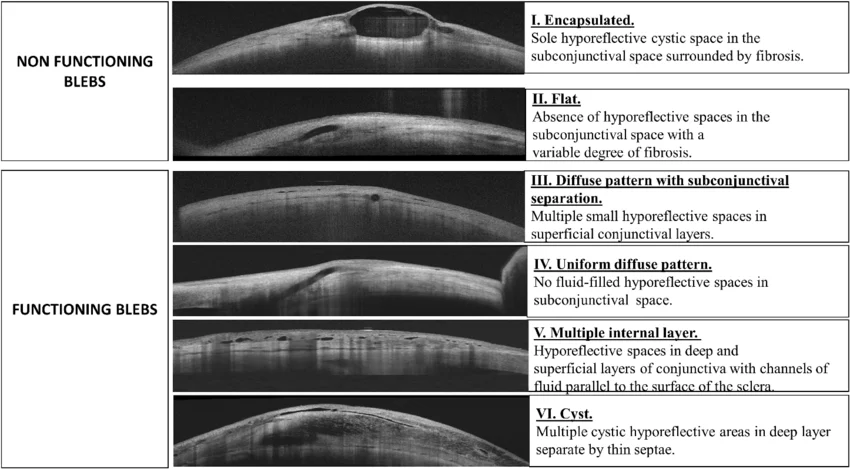
Figure 3: AS OCT based Bleb grading appearance. (5)
Comparing the Grading Systems
| Feature | Würzburg | IBAGS | MBGS | Imaging-based |
|---|---|---|---|---|
| Reference photos | No | Yes | Yes | Yes (AS-OCT/UBM images) |
| Parameters graded | Height, extent, vascularity, leakage | Height, extent, vascularity, leakage | Area, height, vascularity (central/peripheral), leakage | Internal morphology, fluid pockets, flap position |
| Ease of use | High | Moderate | Moderate–low | Low (requires equipment) |
| Reproducibility | Moderate | Good | Very good | Very good (but less standardised) |
| Clinical adoption | Limited | High | Very high | Growing |
Table 1: This table compares between four grading systems.
Clinical Application of Grading
Bleb grading is not merely an academic exercise; it has direct implications for post-operative clinical management and decision-making.
- Flat, vascular bleb: Often indicative of bleb failure and inadequate filtration, and may warrant interventions such as needling or adjunctive antimetabolite therapy.
- Diffuse, avascular bleb: Generally associated with favourable long-term intraocular pressure (IOP) control and a good surgical prognosis.
- Thin, avascular, cystic bleb: Associated with an increased risk of leakage and late-onset bleb-related infection (blebitis), and may require protective or corrective measures such as lubrication, bandage contact lens application, or surgical revision.
- Encapsulated bleb: Common in the early postoperative period and may respond to conservative management such as digital massage or 5-fluorouracil (5-FU) injection.
Standardised bleb grading facilitates consistent interpretation of bleb morphology and supports uniform clinical decision-making across surgeons and institutions.
Limitations of Current Systems
Despite significant advances, existing grading systems continue to face several limitations:
- Subjectivity: Even with the use of photographic reference scales, interobserver variability persists due to differences in clinical interpretation.
- Time constraints: Comprehensive grading systems may be time-consuming and less practical in high-volume clinical settings.
- Incomplete structural assessment: Slit-lamp–based grading primarily evaluates external morphology and does not capture subsurface features that are critical to bleb function.
- Temporal variability: Bleb morphology is dynamic and may change over short periods; thus, grading represents only a single time-point assessment rather than continuous behaviour.
Future Directions
The future of bleb grading is expected to integrate conventional clinical examination with advanced imaging modalities and computational approaches, including Artificial Intelligence (AI), to improve objectivity and predictive accuracy.
- AS-OCT–based grading: AS-OCT enables objective quantification of bleb parameters such as cavity height, cross-sectional area, internal reflectivity, and subconjunctival fluid distribution, offering a more reproducible structural assessment.
- Machine learning applications: AI-driven image analysis has the potential to automate bleb evaluation, reduce interobserver variability, and identify subtle imaging patterns associated with surgical success or failure.
- Integrated multimodal scales: Combining slit-lamp–based morphological assessment with imaging-derived structural and vascular parameters may provide a more comprehensive and accurate prediction of bleb function and long-term survival. Emerging evidence suggests that slit-lamp grading systems (MBGS/IBAGS) and AS-OCT may provide complementary information for more robust and objective outcome assessment. (6,7)
Conclusion
The bleb grading system represents a critical component of postoperative assessment in Glaucoma filtration surgery. From early structured approaches such as the Würzburg classification to widely adopted systems including IBAGS and MBGS, bleb grading has significantly improved the evaluation of surgical outcomes, prediction of bleb survival, and communication of clinical findings.
Despite these advances, current grading systems remain limited by interobserver variability and their inability to capture subsurface bleb architecture. However, emerging technologies such as anterior segment imaging and artificial intelligence–based image analysis are expected to further enhance and potentially redefine bleb assessment in the future.
At present, MBGS and IBAGS remain among the most validated and clinically practical tools for bleb assessment, ensuring that evaluation is guided by structured and reproducible criteria rather than subjective interpretation alone.
A thorough understanding of these grading systems is essential for Ophthalmologists involved in Glaucoma surgery, as accurate bleb assessment is fundamental to optimising surgical outcomes and minimising the risk of vision-threatening complications.
References
- Kahook MY, Schuman JS, Noecker RJ, et al.;Würzburg bleb classification system: a new clinical grading tool for filtering blebs after glaucoma surgery.;Ophthalmology. 2006;113(5):808–813. doi:10.1016/j.ophtha.2005.11.047.
- Cantor, Louis & Mantravadi, Anand & Wudunn, Darrell & Swamynathan, Kala & Cortes, Arnold. (2003). Morphologic Classification of Filtering Blebs after Glaucoma Filtration Surgery: The Indiana Bleb Appearance Grading Scale. Journal of glaucoma. 12. 266-71. 10.1097/00061198-200306000-00015.
- Wells AP, Crowston JG, Marks J, Kirwan JF, Smith G, Clarke JC, Shah R, Vieira J, Bunce C, Murdoch I, Khaw PT. A pilot study of a system for grading of drainage blebs after glaucoma surgery. J Glaucoma. 2004 Dec;13(6):454-60. doi: 10.1097/00061198-200412000-00005. PMID: 15534469.
- Robert L stamper, Marc F Lieberman, Michael V Drake. Becker shaffer’s diagnosis and therapy of the Glaucomas, 8th ed, China; 2009, chapter 34, glaucoma outflow procedure; p 466-490.
- Buenasmañanas-Maeso M, Perucho-Martínez S, Monja-Alarcón N, Toledano-Fernández N. Impact of Primary Needling on the XEN Implant Clinical Outcomes: A Real-Life Retrospective Study. Clin Ophthalmol. 2022 Mar 28;16:935-946. doi: 10.2147/OPTH.S357575. PMID: 35368242; PMCID: PMC8974446.
- Tan S, E L, Husain R, Gazzard G;Anterior segment OCT assessment of trabeculectomy blebs and correlation with clinical grading. Eye (Lond). 2020;34(12):2245–2253. doi:10.1038/s41433-020-0860-2.
- Sugiyama T, Takahashi H, Tomidokoro A.;Relationship between slit-lamp bleb grading and anterior segment OCT parameters after trabeculectomy.;Invest Ophthalmol Vis Sci. 2023;64(7):18. doi:10.1167/iovs.64.7.18.
About the Author

Saptarshi Mukherjee
Saptarshi completed his Bachelor of Optometry from the WBUT, West Bengal, and subsequently pursued a fellowship at Dr. Shroff’s Charity Eye Hospital (SCEH), New Delhi, where he was awarded the Best Fellow distinction. He holds a Master of Optometry from VMU, Tamil Nadu, and has specialized training in glaucoma.
He has authored several research publications and holds NIDA certification for clinical trials. His clinical and research interests include diagnostic, behavioural, Glaucoma and neuro-optometry. He currently serves as a Senior Optometrist at Centre for Sight, New Delhi, and is voluntarily involved as an educator and trainer in the field of optometry. He also serves as Director of Advanced Studies (India) at Vision Science Academy, contributing to the advancement of education and research in vision science.
Recent Comments